Species: Cat, domestic shorthair, 12 years.
Diagnosis: Spinal cord: Severe, acute, focally-extensive myelomalacia and multifocal subdural hemorrhage
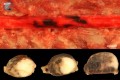
Description: Top (thorakal spinal cord): From T8 to T11 the spinal cord had areas of multifocal to coalescing, blackish-red, subdural discolorations. Bar: 0.5 cm.
Bottom (lumbar spinal cord): Cross sections of segments L3 to L5 revealed multifocal to coalescing predominantly leftsided areas of blackish-red discoloration and softening of the grey and white matter. Bar: 0.5 cm.
Comments: Following a history of hypertrophic cardiomyopathy, the cat presented with clinical symptoms of spontaneous bilateral hind-limb paraplegia, leading to the presumptive diagnosis of aortic thrombosis and/or myelopathy in the thoracic or lumbar regions. However, defecation and micturition were unimpaired. The cat died spontaneously.
Necropsy revealed multifocal to coalescing, acute, subdural hemorrhage as well as hemorrhage and malacia in the grey and white matter of the spinal cord, all of which were moderately present in the thoracic and severely present in the affected lumbar spinal cord regions. Histology additionally revealed multifocal fibrocartilaginous emboli as the probable cause of infarction.
Necropsy also verified severe myocardial hypertrophy of the left ventricle with mild dilatation of the right ventricle with subsequent aortic thrombosis. Additionally, mild general cyanosis, anemia and bilateral adenomas of the thyroid gland were present. Further lesions included moderate, multifocal, chronic, lymphoplasmacytic and fibrosing interstitial nephritis with moderate, multifocal, segmental necrosis and beginning glomerular sclerosis.
The pathomechanism of fibrocartilaginous embolism is still unclear. Most authors assume that fibrocartilaginous emboli start off from the intervertebral disks by herniation of the nucleus pulposus into the vertebral body with subsequent entrance into the internal vertebral vessels.
Etiologic differentials for spinal cord ischemia and necrosis include thrombembolism and bacterial, parasitic, neoplastic, or fat emboli. Predisposing conditions of embolization or thrombosis, such as cardiomyopathy, hyperthyroidism, chronic renal failure –all of which were present in this case – and hyperadrenocorticism or hypertension, should be considered.